

Introduction: The malignant clonal cell proliferation in multiple myeloma (MM) results in significant immune dysregulation through clonal specific T cell expansion, elevated levels of CD4+ CD25+FOXP3+ T regulator cells, downregulation of NK cells, high levels of IL-6 and activation of immunosuppressive tumour associated macrophages (TAM) .
However, the mechanisms underlying the hypercoagulable state in MM and predisposing to venous thromboembolic (VTE) complications is unclear. Confounding disease factors is the use of immunomodulatory drugs (IMiDs) such as Lenalidomide, Thalidomide and Pomalidomide causing ubiquitination and degradation of the Ikaros Family Zinc Finger Protein (IKZF)1 and 3 by cereblon which also contributes to the prothrombotic effect despite thromboprophylaxis.
Aims: The aim of this study was to analyse the changes in the coagulation profile and plasma cell disease burden with treatment, including Lenalidomide, in patients with MM to help define potential underlying mechanisms for hypercoagulability and thrombosis.
Methods: Coagulation profiles and disease markers were retrospectively analysed in 16 MM patients receiving treatment with Daratumumab, Lenalidomide and Dexamethasone (DRd) at The Alfred Hospital, Melbourne from April 2019 to August 2020. Patients enrolled were transplant eligible with MM that was refractory to initial induction therapy with Velcade, Cyclophosphamide and Dexamethasone (VCD). This study was approved by The Alfred Hospital ethics committee.
Statistical analysis was performed using descriptive statistics and the Wilcoxon Sign Rank Test to compare the median coagulation profiles and disease markers after 1-2 cycles of DRd and 3-4 cycles of DRd. Biomarkers included Prothrombin Time (PT), Partial Thromboplastin Time (PTT), Fibrinogen, Thrombin Clotting Time (TCT), serum paraprotein (SPEP) and serum free light chain (SFLC) with a p value of <0.05 indicating statistical significance.
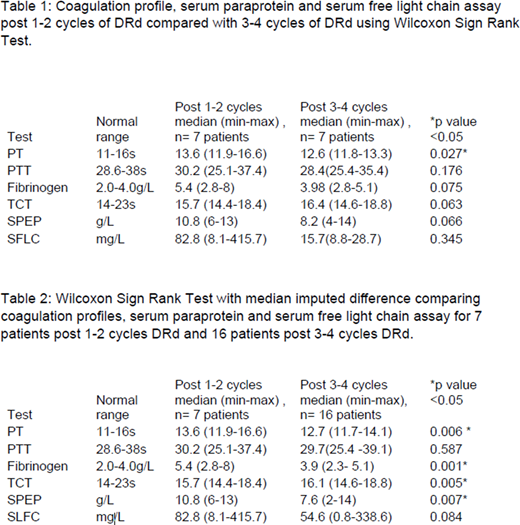
Results: A total 7 patients had coagulation profiles at the two time points i) post 1-2 cycles and ii) post 3-4 cycles of DRd (Table 1). 9 patients had coagulation profiles only after 3-4 cycles of DRd. A separate analysis was performed using Wilcoxon Sign Rank with imputed median differences to allow the inclusion of the 9 additional patients subsequently increasing the sample size to a total of 16 (Table 2). All patients were on anticoagulation with aspirin (n=14), rivaroxaban (n=1) or clopidogrel (n=1) at the time of the analysis.
The analysis showed a statistically significant reduction in PT from median 13.6s (11.9-16.6) to 12.7s (11.7-14.1) with 3-4 cycles DRd in both analysis (p=0.006 and p= 0.027). Fibrinogen levels reduced from median of 5.4 g/L (2.8-8) to 3.98 g/L (2.3- 5.1) after 3-4 cycles (p=0.001). TCT increased after 3-4 cycles of DRd (p=0.005). Serum paraprotein demonstrated statistically significant reduction from 10.8g/L (6 -13) to 7.6 g/L (2-13) after 3-4 cycles (p=0.007). Serum free light chain assay also demonstrated reduction in median values from 82.8mg/L (8.1 - 415.7) to 54.6mg/L (0.8 - 338.6) but was not statistically significant (p=0.084).
Discussion: All the patients in this study either responded to treatment or had stable disease after treatment with DRd. The data demonstrate a coagulation response to treatment. The median fibrinogen level that was above the upper limit of normal declined on treatment, the TCT increased and the PT decreased, all coinciding with the statistically significant decline in paraprotein level. A larger study is required to confirm these findings. However, this study has demonstrated that the hypercoagulable state in MM improves with disease response.
Spencer:Roche: Consultancy, Honoraria; Pfizer: Consultancy, Honoraria; Pharmamar: Other; Secura Bio: Consultancy, Honoraria; Sanofi: Consultancy, Honoraria; Servier: Consultancy, Other: Grant/Research Support; Janssen: Consultancy, Honoraria, Other: Grant/Research Support, Speakers Bureau; Haemalogix: Consultancy, Honoraria, Other: Grant/Research Support; BMS: Honoraria, Other: Grant/Research Support, Research Funding, Speakers Bureau; TheraMyc: Consultancy, Honoraria; Amgen: Consultancy, Honoraria, Other: Grant/Research Support; Takeda: Honoraria, Other, Speakers Bureau; Antegene: Consultancy, Honoraria; Abbvie: Consultancy, Honoraria, Other: Grant/Research Support.

